Fill Your Connecticut Uc 2 Form
The Connecticut UC 2 form serves as a vital tool in the realm of public health, particularly in the surveillance and reporting of sexually transmitted diseases (STDs). Designed to gather comprehensive demographic information, this form captures essential patient details such as name, date of birth, and contact information, ensuring that health officials can effectively track and manage STD cases. Additionally, it provides space for recording critical disease data, allowing healthcare providers to specify reportable diseases like syphilis and gonorrhea, as well as voluntary conditions such as genital herpes. The form also includes sections for laboratory data, detailing the diagnostic tests conducted and their results, thereby facilitating a thorough understanding of each patient's health status. Treatment history is another crucial aspect, where providers can document previous and current treatment methods, offering insights into the effectiveness of care received. By compiling this information, the UC 2 form not only aids in individual patient management but also contributes to broader public health initiatives aimed at controlling and preventing the spread of STDs in the community.
Documents used along the form
The Connecticut UC 2 form is essential for reporting morbidity related to sexually transmitted diseases. However, there are several other forms and documents that often accompany it, providing additional information or serving related purposes. Understanding these documents can help streamline the reporting process and ensure that all necessary data is collected efficiently.
- Patient Consent Form: This document is crucial for obtaining permission from the patient to share their health information. It outlines the purpose of the data collection and explains how the information will be used, ensuring that patient privacy is respected.
- Operating Agreement Form: For forming a robust LLC framework, consult the key Operating Agreement document guidelines to outline essential operating procedures and member responsibilities.
- Laboratory Test Request Form: This form is used to request specific tests from a laboratory. It includes details such as the patient's information, the tests needed, and any relevant medical history. Accurate completion helps ensure timely and correct testing.
- Follow-Up Care Plan: After the initial diagnosis, a follow-up care plan outlines the necessary steps for ongoing treatment and monitoring. It may include recommendations for further testing, treatment options, and referrals to specialists if needed.
- Insurance Claim Form: This document is often required to process insurance claims for the services rendered. It includes details about the patient, the procedures performed, and the costs associated with treatment, facilitating reimbursement from insurance providers.
By familiarizing yourself with these additional forms, you can enhance the overall effectiveness of the reporting process. Each document plays a vital role in ensuring comprehensive care and accurate data management in the context of STD reporting and treatment.
Preview - Connecticut Uc 2 Form
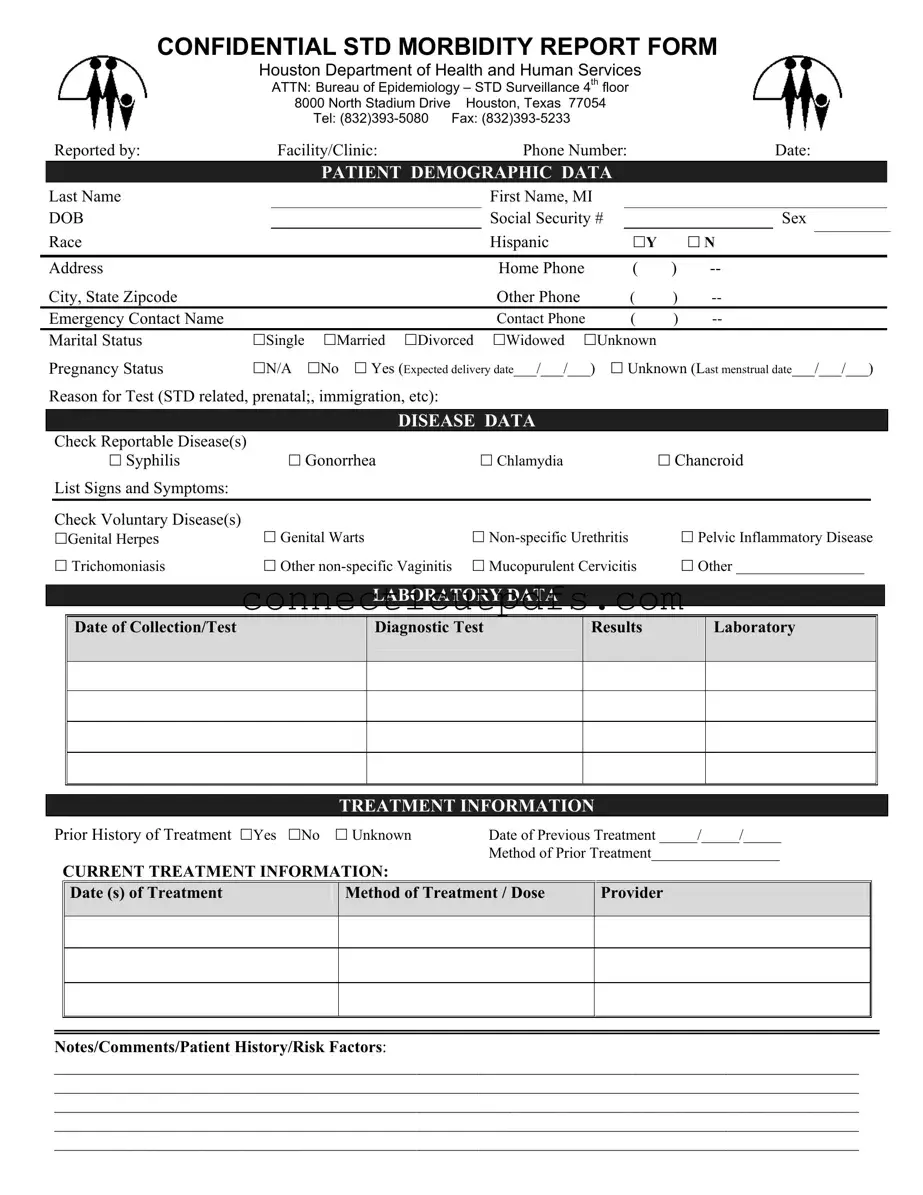
CONFIDENTIAL STD MORBIDITY REPORT FORM
Houston Department of Health and Human Services
ATTN: Bureau of Epidemiology – STD Surveillance 4th floor
8000 North Stadium Drive Houston, Texas 77054
Tel:
|
|
Reported by: |
|
Facility/Clinic: |
|
Phone Number: |
|
|
Date: |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
PATIENT DEMOGRAPHIC DATA |
|
|
|
|
|
|
|||||
|
Last Name |
|
|
|
|
|
First Name, MI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DOB |
|
|
|
|
|
Social Security # |
|
|
|
Sex |
|
||||
|
Race |
|
|
|
|
|
Hispanic |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Y |
|
N |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Home Phone |
( |
) |
|
|
|
|
|||
|
City, State Zipcode |
|
|
|
|
|
Other Phone |
( |
) |
|
|
|
|
|||
|
Emergency Contact Name |
|
|
|
|
|
Contact Phone |
( |
) |
|
|
|
|
|||
|
Marital Status |
Single |
Married |
Divorced |
Widowed |
Unknown |
|
|
|
|
|
|
||||
|
Pregnancy Status |
N/A |
No |
Yes (Expected delivery date___/___/___) |
|
Unknown (Last menstrual date___/___/___) |
|
|||||||||
|
Reason for Test (STD related, prenatal;, immigration, etc): |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISEASE DATA |
|
|
|
|
|
|
|
|
|
|
|
Check Reportable Disease(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Syphilis |
|
|
Gonorrhea |
|
Chlamydia |
|
|
Chancroid |
|
|||||
|
|
List Signs and Symptoms: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check Voluntary Disease(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Genital Herpes |
|
Genital Warts |
|
|
|
Pelvic Inflammatory Disease |
|
|||||||
|
|
Trichomoniasis |
|
Other |
Mucopurulent Cervicitis |
|
Other _________________ |
|
||||||||
LABORATORY DATA
Date of Collection/Test
Diagnostic Test
Results
Laboratory
TREATMENT INFORMATION
Prior History of Treatment Yes No |
Unknown |
Date of Previous Treatment _____/_____/_____ |
|
||
|
|
|
Method of Prior Treatment_________________ |
|
|
|
CURRENT TREATMENT INFORMATION: |
|
|
|
|
|
Date (s) of Treatment |
Method of Treatment / Dose |
Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notes/Comments/Patient History/Risk Factors:
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Common Questions
What is the Connecticut UC 2 form?
The Connecticut UC 2 form is a confidential morbidity report used to document and report cases of sexually transmitted diseases (STDs) to the appropriate health authorities. This form is essential for public health surveillance and helps in tracking the incidence of STDs in the community.
Who should fill out the UC 2 form?
The UC 2 form should be completed by healthcare providers, clinics, or facilities that diagnose or treat patients with reportable sexually transmitted diseases. This includes doctors, nurses, and other medical professionals involved in patient care.
What information is required on the UC 2 form?
The form requires various types of information, including patient demographics such as name, date of birth, and contact information. It also asks for details about the reportable disease(s), laboratory test results, treatment history, and any signs or symptoms the patient may have experienced.
How is patient confidentiality maintained when using the UC 2 form?
Patient confidentiality is a priority when completing the UC 2 form. The form is designed to be confidential, and any identifying information is handled in accordance with health privacy laws. Healthcare providers must ensure that the form is submitted securely to protect patient information.
What diseases are reportable on the UC 2 form?
The UC 2 form includes several reportable diseases such as syphilis, gonorrhea, and chlamydia. Additionally, it allows for the reporting of voluntary diseases like genital herpes and pelvic inflammatory disease, among others. Providers should check all applicable diseases on the form.
What should be done if a patient has a history of treatment?
If a patient has a prior history of treatment for an STD, this should be noted on the UC 2 form. The form includes a section for documenting the date of previous treatment and the method used. This information can be crucial for understanding the patient's current health status and treatment needs.
How can the UC 2 form be submitted?
The completed UC 2 form can be submitted via fax or mail to the Bureau of Epidemiology at the Houston Department of Health and Human Services. The contact information for submission is provided on the form itself. It is important to ensure that the form is sent securely to maintain confidentiality.
What if the patient is unsure about their pregnancy status?
If a patient is unsure about their pregnancy status, the healthcare provider should select the "Unknown" option on the UC 2 form. This allows for accurate reporting while acknowledging that not all patients may have definitive information regarding their pregnancy.
Can additional notes be added to the UC 2 form?
Yes, there is a section on the UC 2 form for notes and comments. This area allows healthcare providers to include any relevant patient history, risk factors, or additional information that may assist in the understanding of the patient's condition and treatment.
What should a provider do if they have questions about completing the UC 2 form?
If a provider has questions about how to complete the UC 2 form, they can contact the Bureau of Epidemiology at the Houston Department of Health and Human Services. The contact number is provided on the form, and staff are available to assist with any inquiries related to the reporting process.
Common PDF Forms
Connecticut Fpd 124 - Identification details for sellers and pledgers are required on the form.
For those looking to navigate the complexities of property transactions, a reliable resource is the comprehensive guide for the Bill of Sale that can be found here.
How to Become a Teacher in Connecticut - The ED 170 form is the official application for certification in Connecticut’s education system.
Guide to Filling Out Connecticut Uc 2
After completing the Connecticut UC 2 form, it will be submitted to the appropriate health department for processing. Ensure that all required information is accurate and complete to avoid delays in handling the report.
- Begin by filling in the Reported by section with your facility or clinic's name and phone number.
- Enter the Date of the report.
- In the PATIENT DEMOGRAPHIC DATA section, provide the patient's last name, first name, and middle initial.
- Fill in the DOB (Date of Birth) and Social Security #.
- Indicate the patient's Sex and Race.
- Specify if the patient is Hispanic (Yes or No).
- Complete the Address, including city, state, and zip code.
- List the Home Phone and any Other Phone numbers.
- Provide the Emergency Contact Name and their phone number.
- Indicate the patient's Marital Status (Single, Married, Divorced, Widowed, Unknown).
- Specify the Pregnancy Status (N/A, No, Yes, Unknown) and include relevant dates if applicable.
- State the Reason for Test (e.g., STD related, prenatal, immigration).
- In the DISEASE DATA section, check all applicable Reportable Disease(s) such as Syphilis, Gonorrhea, Chlamydia, and Chancroid.
- List any Signs and Symptoms observed.
- Check any Voluntary Disease(s) that apply, including Genital Herpes, Genital Warts, and others.
- In the LABORATORY DATA section, provide the Date of Collection/Test and the Diagnostic Test Results.
- Enter the name of the Laboratory that conducted the tests.
- For TREATMENT INFORMATION, indicate if there was a Prior History of Treatment (Yes, No, Unknown) and provide the date and method if applicable.
- For CURRENT TREATMENT INFORMATION, list the Date(s) of Treatment and the Method of Treatment / Dose.
- Finally, include any Notes/Comments/Patient History/Risk Factors relevant to the case.
Dos and Don'ts
When filling out the Connecticut UC 2 form, it is essential to ensure accuracy and completeness. Here are five important dos and don'ts to keep in mind:
- Do provide accurate patient demographic data, including full names and contact information.
- Do check the appropriate boxes for reportable and voluntary diseases to ensure proper reporting.
- Do include the reason for the test clearly to help with understanding the context of the report.
- Do document any previous treatments and their details accurately to maintain a comprehensive medical history.
- Do ensure that all dates, especially those related to treatment and tests, are filled out correctly.
- Don't leave any sections blank; incomplete forms can lead to delays in processing.
- Don't use abbreviations or shorthand that may confuse the reader.
- Don't provide false or misleading information; honesty is crucial for patient care.
- Don't forget to include emergency contact information, as it may be vital in urgent situations.
- Don't overlook the importance of legibility; ensure that handwriting is clear if the form is filled out by hand.